

Definition
A Retinopathy of prematurity is a disease resulting from the interruption of the normal vascularization of the retina.
If birth occurs prematurely, the normal growth of retinal blood vessels is interrupted. When it proceeds some weeks after birth, it may become disorganized with the formation of abnormal vessels, which lead to severe alterations in the structure of the retina and eventually to blindness in the most serious cases.
Is it an eye disease that affects only prematurely-born babies? Why?
As the name itself specifies, it is a disease that affects only preterm babies.
Retinal vascularization begins around the 12th week of gestation and is only concluded between the 36th and 40th week.
Retinal blood vessels grow due to very complex biochemical stimulation: a substance named VEGF (vascular endothelial growth factor) is the last element in a series of events responsible for their growth. VEGF action depends on the level in the blood of another substance, IGF1 (insulin growth factor), supplied to the foetus through the placenta. When birth occurs prematurely, there is a sudden decrease of the levels of IGF1 with interruption of the stimulation by VEGF. Consequently, retinal vessels stop growing.
This hindrance is many times aggravated by the administration of oxygen in incubators. Oxygen in high concentrations, necessary to keep the baby alive, often contributes to hinder the growth of blood vessels, and it can cause even the regression of some vessels recently developed.
With the baby’s growth, when the levels of IGF1 are reset by the baby’s own production, the extremely high levels of VEGF then accumulated lead to an excessive and uncontrolled growth of abnormal vessels that may result in retinal detachment and blindness.
Which are the factors of risk for the development of this disease?
Retinopathy of prematurity is a multifactor disease.
The main factor of risk is prematurity, expressed by gestation time and weight at the moment of birth: the shorter the time and/or the lower the weight, the greater is the risk. In developed countries with good neonatal care (Portugal included), neonates weighing less than 1500g are particularly at risk of developing retinopathy of prematurity.
Another very important factor of risk is the supplemental oxygen administered to the baby during the first weeks of life. Great fluctuations of oxygen levels in the blood are particularly dangerous for the development of the disease.
Other factors of risk usually considered include sepsis, haemodynamic alterations, multiple blood transfusions, multiparity, hyaline membrane disease, E vitamin deficiency, the use of aminofilina, some antibiotics, low pH, ultraviolet light, etc.
Which is the prevalence of retinopathy of prematurity in Portugal?
There are few studies on retinopathy of prematurity in Portugal. In 2004, a multi-centre study conducted by the Portuguese Society of Neonatology pointed to a prevalence of 20.4%, but concluded that only 66.7% of premature babies at risk were examined by an ophthalmologist. The number of medical examinations per premature child and the experience of the examiner in the diagnosis of this disease were not specified. These two points are fundamental for a correct evaluation of prevalence.
In Hospital São João, we carried out a retrospective study of the cases of premature babies weighing less than 1500g, examined in 2005 and 2006 by one out of two paediatric ophthalmologists with much experience in this area. Besides, all premature babies were repeatedly examined, in accordance with the international protocol, until complete retinal vascularization. This study concluded that the prevalence of retinopathy of prematurity was 61.6% in babies weighing less than 1500g at birth.
Fortunately, the disease did not evolve to severe forms in the great majority of these babies; it reached stage 2 or superior only in 2.7% of the cases.
How is this disease diagnosed?
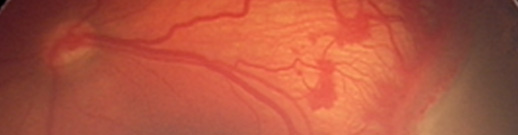
The diagnosis is made by examining the eye fundus of the baby with an indirect ophthalmoscope and a 28 or 30 dioptre lens. Usually this examination is not easy, and so it should be done by an ophthalmologist with much experience in this pathology.
A device to photograph the fundus of babies’ eyes appeared recently on the market.
If images are correctly captured, it enables a distance analysis by an experienced ophthalmologist, through the Web network. This method allows detecting retinopathy of prematurity in babies treated in centres without ophthalmology experts in this disease.
Is it possible to prevent this disease?
The ways to prevent this disease are almost inexistent, as it is essentially due to prematurity.
The possible prevention consists in excellent neonatal care. In developing countries, where this care is not optimal, the prevalence and severity of this disease is greater, even in heavier and more mature babies at preterm birth. Simultaneously, it is fundamental to ensure good haemodynamic equilibrium, by controlling oxygenation and preventing great fluctuations of the oxygen levels.
Above all, it is important to detect the disease in due time, to treat it correctly and at the exact moment.
After the diagnosis, how is retinopathy of prematurity treated?
First of all, treatment necessity is decided based on objective criteria, and only then should it be administered within 48 – 72 hours.
Retinopathy of prematurity is treated with cryotherapy (low temperatures probe) or with laser. Both treatments are ablating, burning part of the avascular retina. This way the stimulus to proliferation of abnormal vessels, capable of destroying normal retina, is reduced.
New methods of treatment are creating now great expectations. One of them consists on an intraocular injection of substances capable of blocking the excessive VEGF and so of controlling the development of abnormal blood vessels.
If the disease has already progressed to retinal detachment, then an intraocular microsurgery is required.
Which are the possible consequences of this disease for the baby?
The first possible consequence results from a severe stage of the disease. When retinopathy does not regress spontaneously or does not respond to treatment, it progresses to retinal detachment, very difficult to treat, and generally leads to blindness.
Medium and long term consequences are mainly a greater incidence of strabismus and refractive errors. Myopia is much more frequent in premature children and even more in those submitted to treatment (especially cryotherapy compared to laser therapy). In treated patients the visual field is a little reduced. In general, premature infants with retinopathy present slightly diminished visual acuity and chromatic vision.
How should parents be advised in order to deal better with this disease?
First of all, parents should be informed about the disease and its nature. They have to realize that premature babies should be appropriately monitored, in due time, by qualified professionals.
Sometimes multiple examinations are necessary, even after the discharge from hospital, and parents should attend all medical interventions.
They should also know that ophthalmological monitoring of premature children does not end when retinal vascularization is complete. Periodic screenings are necessary, according to medical advice, because refractive errors and strabismus occur very frequently.