


Definition
Strabismus is any misalignment of the visual axes. The deviation of one of the eyes may be horizontal (convergent or divergent), vertical (upward or downward) or torsional with a more difficult diagnosis. In practice, the deviations are very often mixed, as the visual axes are misaligned in more than one direction.
Strabismus presents also other forms, more complex and rarer, which are sometimes associated with other ocular or systemic disorders.
Incidence
In Portugal, the number of individuals with strabismus is unknown. Nevertheless, considering that the prevalence of strabismus in populations with demographic characteristics similar to ours is about 3%, we can estimate that in Portugal there are about 320,000 persons with strabismus and that 50,000 of them are children under 14 years of age.
Causes
The causes vary with the type of strabismus, the age at its onset and the demographic characteristics of the population.
In infancy, the most frequent form of strabismus is accommodative endotropia, which represents about 80% of all the cases. It usually appears between 2 and 5 years of age, but it may develop earlier, and it is the result of the child’s effort to focus the images. Though it may be due to an alteration in the relation between accommodation and convergence, in most cases it is caused by uncorrected hypermetropia. This form of strabismus is particularly important because it can be prevented: if the cause is diagnosed and corrected in time, the onset of strabismus and consequent amblyopia (lazy eye) can be avoided. Therefore, at the beginning of the child’s 2nd year of life, visual screenings are of great importance.
The cause of congenital endotropia is still unknown. It appears during the first 6 months of life and it is characterized by a wide angle deviation (many times associated with a vertical deviation).
Another important cause of strabismus is the impaired vision of one of the eyes – sensory strabismus. The existence of cataract, detached retina or another serious origin of hypovision can cause a deviation of the affected eye.
Except for sensory exotropia, the cause of divergent deviations is not very well known. Many times an initial divergence, with progressive deterioration of the capacity to fuse images from the two eyes, develops into the settling of a constant deviation.
There are several factors of risk associated with the onset of strabismus. Besides children with a family history, those with a greater risk to develop strabismus are: premature babies with a gestation age below 28 weeks and/or with less than 1500g at birth; children with perinatal complications involving the central nervous system or with retarded development; and also infants with some genetic syndromes, especially those associated with craniofacial alterations.
Diagnosis
As the causes, the symptoms depend on the type of strabismus, the age at its onset and the way it settles in.
In children, especially the youngest ones who do not verbalize, symptomatic complaints are many times inexistent, and so the signs resulting from the infant’s adaptation are very important.
The most evident sign is the ocular misalignment itself. When the deviation occurs, there is a duplication of the images – diplopia. In adults, this diplopia persists as long as the deviation exists. In children, however, this process evolves differently: to have a comfortable vision, they quickly develop a mechanism of “suppression” of the second image. This mechanism leads to not using one of the eyes, and in the absence of treatment it will have consequences at the level of the visual cortex, with the development of amblyopia.
Before this suppression becomes permanent, the child may close the deviated eye to avoid diplopia: a sign that should always be considered important in a child.
Some types of strabismus can be compensated by changing the position of the head.
A torticollis should always be evaluated by an ophthalmologist, in order to detect any alteration in the ocular motor equilibrium.
The presence of non-compensated strabismus always impairs binocular vision, with a deficient or inexistent reaction in stereopsis tests.
|
Symptoms of strabismus
|
Signs of strabismus
|
|
Diplopia
|
Ocular misalignment
|
|
Amblyopia
|
Shutting an eye
|
|
Reduced stereopsis
|
Torticollis
|
A simple screening test for strabismus consists in projecting a light onto the child’s eyes and checking if the reflection is centred in the two eyes. See illustrations below (pictures 1 to 3).
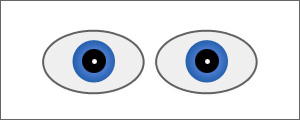
Picture 1 – The reflections are centred. Inexistence of strabismus.
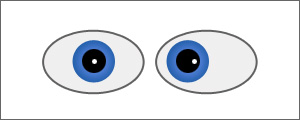
Picture 2 – The reflection of left eye, is deviated outwards: convergent strabismus
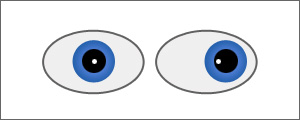
Picture 3 – The reflection of left eye, is deviated inwards: divergent strabismus.
Pseudostrabismus
Pseudostrabismus or false strabismus is very frequent, above all in very young infants. Although the child seems to have strabismus (usually convergent), in fact the eyes are well aligned.
This false appearance of strabismus is produced by the minute portion of sclera visible on the nasal side of the eyes. In general, this is due to the existence of prominent epicorners, a wide nasal bridge, or alterations of the interpupillary distance.
Treatment
After diagnosing strabismus, the main concern is to evaluate thoroughly the clinical condition of the patient, in order to determine the cause or causes, the factors of risk associated and the consequences of the deviation.
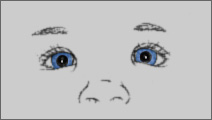
Picture 4 – The existence of folds in the inner corner of the eyes (epicorner) and the wide base of the nose give a false sensation of strabismus. Nevertheless, the presence of centred reflections demonstrates the inexistence of a misalignment.
The correction of possible underlying causes is more urgent than the treatment of the deviation itself. For instance, all significant refractive errors should be corrected. Many cases of strabismus are treated with the prescription of appropriate corrective glasses.
Among the consequences of strabismus is amblyopia, particularly important. Whenever advised, glasses are fundamental but many times insufficient for the treatment. It is then necessary to “disable” the dominant eye, for instance by using eyepatches or instilling drops to lessen temporarily the sight of that eye, or to apply a therapy to stimulate sight.
It is important to stress that all these treatments are intended to improve the visual function and not to cure strabismus!
Finally, the deviation itself, which persists after the optical correction, can be treated by surgery. In some cases, an alternative to surgical treatment is to apply injections of botulinal toxin in the extraocular muscles.